Not to be outdone, Kola has been busy in Liberia with neonatal resuscitation training at the same time as the Cameroonian course was running. WhatsApp was alive with photos coming in for a couple of days – heartening stuff to our NICHE team still unable to leave the UK to train more instructors.
Neonatal technicians in Liberia lecturing on Newborn Life Support during a resuscitation training session, June 2021
Learning Curve: shows a relationship between the amount of practice / experience of a skill and the degree of competence achieved.
Forgetting Curve: the relation between the decay of a learned skill and the time elapsed since the skill was learned.
Experience Curves: combines the learning and forgetting curves.
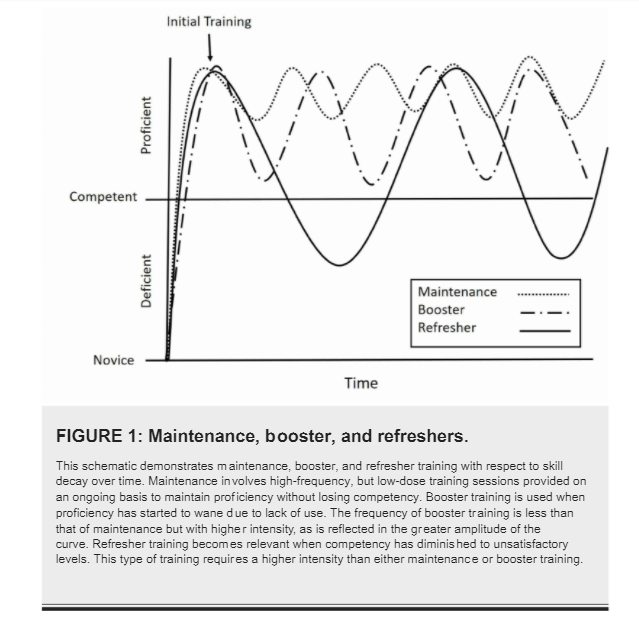
Activities to overcome skill decay can be qualitatively classified as maintenance , booster or refresher, according to the diagram below:
Note the amount of time spent “deficient” with “refresher” activities. An example of this is paediatricians in the UK re-certifying in APLS every 4 years. “Booster” training is possibly achieved by statutory mandatory training paediatric basic life support every year and keeps the average paediatrician “proficient”. Would lower intensity but more frequent “maintenance” activities do a better job eg. weekly simulation training sessions?
Here is Kola delivering his “booster” training sessions in neonatal resuscitation to nurse technicians in Liberia this week, using equipment left by NICHE after the first batch of instructors were trained in 2019.
Kola (centre) teaching neonatal resuscitation in Liberia, February 2021
How often does he need to run these sessions to make this maintenance training and not refresher sessions? The quest continues….
Medical and nursing staff in the UK now have to undergo annual appraisals, usually with a peer who coaches them through their appraisal paperwork, discussing issues and highlights of the year with them and helping them to develop themselves as a health professional. Although there’s always a mad rush at the end of the year to get all the relevant bits of paper uploaded to one’s appraisal file in time for the allotted meeting, the process if done well encourages the health worker to focus on their goals for the next year, helps to prevent burn out and allows us all the space to reflect on our own practice.
Agnes, instructor in Liberia
This process is in its infancy in Liberia and Cameroon. Jarlath has put together a draft form which gathers information about skills and confidence decay, provides a method of assessing someone’s on-going competence and allows a structure for peer mentoring. We are not quite sure how this will work in the field but will be rolling it out over the next few years in Cameroon while we work out how to help support local instructors in the long term.
WHO suggests that babies should be exclusively breastfed for the first 6 months of life. UNICEF data for Liberia for 2013 suggests that 55% of babies 0-5 months of age are exclusively breastfed although it’s only 34% for the whole West African region:
I can’t find the accurate figure of percentage of babies who are still being exclusively breastfed at 6 months of age in Liberia but it might be around 20%. We’ve been hearing today that lots of babies get “gripe water” in the first few days of life. I think it still has alcohol in it here. Besides formula, they are also fed corn and rice cereals from a very young age.
Breastfeeding should be initiated within the first hour of birth and one of the issues in Liberia which might be contributing to the poor breastfeeding rates is the birth practice which removes the baby from the mother for the first vital minutes to clean and dress it. Instead of this, the newborn – whilst being kept warm of course – should be delivered on to the mother’s abdomen, dried except for the hands and he/she will “commando crawl” up to the breast on its own. This is shown beautifully in one of the excellent Global Media videos that I’ve mentioned before. Have a look at it here: https://globalhealthmedia.org/portfolio-items/early-initiation-of-breastfeeding/?portfolioCats=191%2C94%2C13%2C23%2C65. We played this video to the learners (who were all midwives) on the first Newborn Care Course earlier this week. They went away with good intentions to change their practice. I think it could do with being shown in a few centres in the UK too.
One of the slides from the NCC lecture on Nutrition and Feeding
This is a slide from one of the early lectures on the Newborn Care Course. It outlines WHO’s priorities in the fight to bring down neonatal mortality (number of deaths per 1,000 live births) to “at least as low as 12 per 1,000” by 2030.
Liberia’s neonatal mortality rate is 25 per 1,000 [UNICEF 2018 data]. 3 babies have died in the hospital in Zwedru since we’ve been here; 2 term babies born with severe hypoxic ischaemic encephalopathy (lack of oxygen around the time of birth) and 1 preterm baby weighing 900g who looked quite well when we arrived but died on day 6 of life during our second course – despite 2 of the local instructors leaving the course to go to the hospital to try and help save the baby.
Not many babies under 1.5kg survive here. Kola’s been discussing this this evening and showing us pictures of his successes – including one little lad called Success, born by perimortem Caesarean section to a mother with severe eclampsia, at 1kg. Now, developmentally normal and with adoptive parents, the family recently came back to the unit to celebrate his second birthday. Kola’s smallest survivor weighed just 600g at birth at 29 weeks gestation. He is now over 1 and also developmentally normal. I suspect that although the survival rates at different gestational ages are very much lower than in the UK, the percentage surviving without severe disability is probably higher.
Kola’s turns of phrase when he’s lecturing have been delighting Jo and I all day. The title of this and the previous posts are good examples of the fervour with which he plays his role as MCAI’s on the ground neonatal trainer. And he is not alone. Gertrude, Agnes and Christina are equally dedicated to their patients and their unit, totally committed to the patients they look after. And totally engaged in their roles today as instructor candidates on the Newborn Care Course.
Gertrude doing Stage 2 of the 4-stage procedure in how to tie a kalafong wrap for the baby to be skin-to-skin with its mother.
Christina overseeing resuscitation skills training.
Agnes (gesticulating with her hands) running an animated discussion workshop on pain in babies and how to manage the baby who won’t live long.
Here are our 4 local instructors with their certificates of completion of the Generic Instructor Course in Zwedru. Well deserved. They put so much energy into the course and really developed as teachers over the 2 days.
And here are the 5 newly trained instructors in Monrovia where Colin and Alistair are running parallel courses to Jo and Julia. 1 X GIC followed by 2 x NCCs.
These neonatal clinicians and 1 doctor now have to teach on two Newborn Care Courses supervised in order to complete their training as instructors. The NICHE International volunteer instructors should be able to complete this whole process in the one 10-day trip. We will also be leaving a teaching set (4 manikins, scenario teaching sets and a projector) with the new Liberian faculty so that they can start to organise and run their own courses. It would be nice to be invited back to help out though!
We have been teaching the Generic Instructor Course today, one of the best train the trainer short courses in the world I think and it travels well. We learnt about Maslow’s hierarchy of needs in one of the sessions.
Maslow (1943) divided this five-stage model into deficiency needs and growth needs. The first four levels are often referred to as deficiency needs (D-needs), and the top level is known as growth or being needs (B-needs).
Deficiency needs arise due to deprivation and are said to motivate people when they are unmet. Also, the motivation to fulfill such needs will become stronger the longer the duration they are denied. For example, the longer a person goes without food, the more hungry they will become.
We had a beautiful example of this here in Liberia where our learners have been a bit vexed by a misunderstanding over food provision during the courses. They were hoping to get money to buy their food with (and no doubt save some of the money out of this allowance) and were not pleased to find out that “their” food money had been given to caterers to provide the food. This was compounded when the caterers failed to turn up with the food! Jo and I were trying to persuade them to prepare for the GIC course over the weekend but they could not do that because they were still animatedly discussing the issue around food allowances. It was not until that issue had been sorted out this morning that they could start to move up Maslow’s pyramid. In one day we’ve gone from level 1 to level 4 and will nudge our learners into level 5 by (complimentary) morning coffee tomorrow.
In Liberia the climate is tropical, hot and humid all year round, with a rainy season from May to October due to the African monsoon, and pretty frequent rains in the other months, except in the short dry season that runs from December to February. This makes for a green, lush environment in most of the country as we found out on our evening walk earlier.
The rains have gone on longer than usual this year and this picture from the Liberian Observer shows just how bad the road is from the capital to the county in which we are based currently.
The health professionals coming to our Newborn Care Courses this week have to travel this road. On motorbikes apparently because the cars that were supposed to be bringing them can not get through.
This evening, I was admiring the sunset from the UNHCR compound where we are staying. The next thunderstorm is obvious on the horizon in this picture and is just breaking now as we are going to bed. The rain on the corrugated iron roof is deafening and there is a leak in the ceiling just above the sofa. How do the children study in the evenings in conditions like this? It makes me think of Maslow’s hierarchy of needs which is one of the topics on tomorrow’s GIC. More about that in tomorrow’s post – if the internet is still working. A lightening strike has damaged our Wifi so we’re reliant on Kola’s data at the moment.










 This is Kola putting his all into his lectures, carrying his learners with him on a wave of enthusiasm. A truly inspirational educator.
This is Kola putting his all into his lectures, carrying his learners with him on a wave of enthusiasm. A truly inspirational educator.




